
PCR test — “Viral culture for every individual case is needed to conclude if the person “presents any danger to society.”
“So what does it take to indicate a true positive COVID test? Simply put, you take a PCR test and if you test positive you are deemed “infectious,” but this is glossing over a myriad of missing facts that desperately need discussion.”
The following is a breakdown on the effectiveness of PCR testing to diagnose COVID-19. I will be relying on primarily three sources of data as a source of reference while writing this article. One is a study from the Centre For Evidence Based Medicine (CEBM), the other is a study from the Journal Of Clinical Virology titled “Real-time PCR-based SARS-CoV-2 detection in Canadian laboratories,” and the last reference will be from a New York Times article titled “Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be.”
Let’s proceed to reference from each source in order starting with the Centre For Evidence Based Medicine study titled “PCR positives: what do they mean?”
“PCR detection of viruses is helpful so long as its accuracy can be understood: it offers the capacity to detect RNA in minute quantities, but whether that RNA represents infectious virus may not be clear.”
So what does it take to indicate a true positive COVID test? Simply put, you take a PCR test and if you test positive you’re deemed “infectious,” but this is glossing over a myriad of missing facts that desperately need discussion.
Testing positive – What does it mean?
You can test positive and not be able to infect anyone with the virus. The test could be picking up dead virus from months ago, but don’t take my word for it, take a look at these quotes from the study.
“Imagine that a virus enters your body. In a few months it might not do anything to you anymore. It might not do anything to your cells (virulence), and it might also lack the capacity to move into another person (infectivity) when you speak or sneeze. It is also possible that this virus simply never did anything to you and lacked infectivity from the very beginning. But traces of the virus might still be present in the person. In this case, the virus is present but inactive.”
So how do you know you’re truly positive (infectious)?
“You do the PCR. If the virus is found in the person (PCR TRUE POSITIVE), that virus is injected into a culture cell. If by injecting that virus into culture cells, the virus is not able to reproduce in the cells, that virus cannot infect anybody any longer. This means that even if you are a PCR positive, you are no longer contagious, that is, the virus in you is no longer active.”
So aren’t we still injecting positive test results (virus) into a culture cell to ensure it’s actually infectious before stealing that person’s charter rights and liberties? Well, here’s some disturbing revelations provided by the National Microbiology Laboratory (NML), who previously conducted this type of testing.
“During the early days of Canada’s response to COVID-19, all laboratory samples were sent to the NML from provincial and territorial public health labs to confirm the presumptive results. Still now, the NML continues to work in close collaboration with these public health labs to ensure that the test we use to diagnose COVID-19 remains accurate.
The NML provides all provinces and territories with laboratory reference services on an ongoing basis. These testing services provide a variety of support to provincial and territorial laboratories across Canada, including confirmatory testing for all presumed positive samples, quality assurance to ensure testing is accurate and in-depth analysis of difficult to diagnose specimens.”
This is the NML essentially admitting that they no longer send these tests off to confirm that the person testing positive can actually infect others. You may not believe me — but let me break down the language.
What is a presumptive case?
A presumptive case according to the CDC is anyone who has tested positive for the virus, but testing was conducted at the local or state level. Currently, presumptive positive cases must have a sample undergo confirmatory testing at the CDC. So a presumptive case is a positive that has yet to be laboratory confirmed.
Back to Canada where the NML has said “during the early days of Canada’s response to COVID-19, all laboratory samples were sent to the NML from provincial and territorial public health labs to confirm the presumptive results. Still now, the NML continues to work in close collaboration with these public health labs to ensure that the test we use to diagnose COVID-19 remains accurate.”
As the NML states above they have the ability to assist with laboratory testing, but it’s very murky whether these local health units are reaching out to confirm results now that they are no longer required too, in addition it’s unclear what percentage are being lab confirmed.
It remains unclear what percentage of our presumptive cases are being sent to the NML to confirm that the person with a positive result (PCR positive) is also infectious. This means people testing positive may be carrying a dead virus or lack the ability to infect others all together!
It gets worse
“Conclusion: A TRUE POSITIVE in PCR does not always mean that the person presents any danger to society. The virus cannot be transmitted when cell culture shows that the virus is not infective. Unfortunately relating PCR POSITIVE to infectivity is not easy if we consider the whole population. This would require 1) a model (correlation) that maps PCR POSITIVES and/or symptoms to infectivity as tested by viral culture or 2) viral culture for every individual case.” This is directly from the study “PCR positives – what do they mean?”
They conclude that viral culture for every individual case is needed to conclude if the person “presents any danger to society.”
How accurate are PCR tests?
Cycle thresholds — “Cycle thresholds are the times that the amplifying test has to be repeated to get a positive result. The higher the viral concentration the lower amplification cycles are necessary.” Some people might give a positive test result after running the PCR test with a high threshold and others with a low threshold.”
This means that depending on the cycle counts of the testing, someone could test positive or negative. Its also worth noting some of the testing centres in Canada aren’t disclosing their cycle count cutoffs, and some run at 35 while others run at 45. The high-end cutoff in the United States is a cycle count of 40. Canada has multiple testing centres that run above this recommended cycle count. This could create two different results within the same individual.

As I continued to read through the study, I began to get more angry at our governments current handling of this “pandemic”.
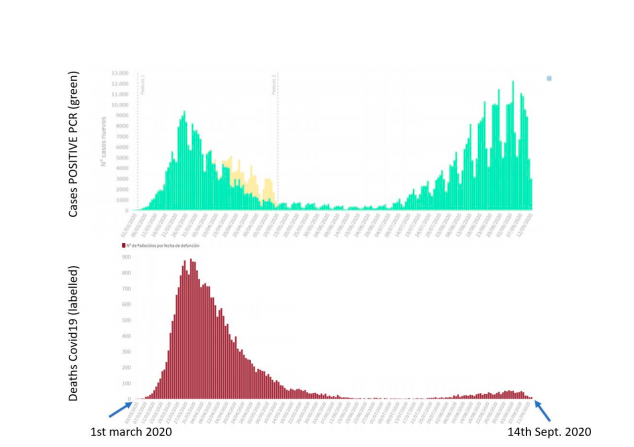
“Calling PCR positives “cases” does not specify whether the persons have carried the virus for long, or whether it is “active”. This could lead to the finding of many “cases” as a function of the number of PCR tests conducted. For example, if 20% of a population are PCR positive, the number of PCR positives will depend on the size of the sample. This means that the more PCR test are carried out the larger the fraction of the population that is confirmed but this might not speak of changes in the population. That is, it is possible that the population was infected already long before deciding to test and PCR positives would therefore not speak of “an advancing pandemic.”
Breaking down case definitions of Ford government
The following points are read directly from the governments definitions of cases.
“A person with laboratory confirmation of SARS-CoV-2 infection using a validated assay, consisting of positive nucleic acid amplification test (NAAT; e.g. real-time PCR or nucleic acid sequencing) on at least one specific genome target. Laboratory confirmation is performed at reference laboratories (e.g., The National Microbiology Laboratory or Public Health Ontario Laboratory) or non-reference laboratories (e.g., hospital or community laboratories) (see footnote 7).
OR
A person with a positive detection of serum/plasma immunoglobulin G (IgG) antibodies to SARS-CoV2 from a laboratory in Ontario that is licensed to conduct serology testing for clinical purposes.”
Notice in the above paragraphs, it doesn’t mention what percentage of test are sent off for laboratory confirmation or what percentage go to what labs. It is also unclear if laboratory confirmation includes injecting the “positive” infection into a cell culture to see if it’s infective. So to be clear, we don’t know what percentage are tested to “verify their infectivity,” and non-reference laboratories are allowed to be used to run these tests?
This is an absolute must — to ensure that a positive test actually means that an individual is able to infect others. Again, don’t take my word for it, “we suggest that the hypothesis of CEBM, i.e. that viral culture is required as a reference to test for infectivity.” —Study: “PCR positives – what do they mean?.”
Send a letter to Premier Ford and attach this article. Ask if the cases being reported are presumptive cases or confirmed cases by the NML. Ask what percentage of current cases are being laboratory confirmed by injecting the virus into cell cultures as NML did to confirm positive test results in early January. You likely won’t get an answer and if you do – you may not like it.
@DivergeMediaNews via Facebook
Diverge Media doesn’t get media bailout money like the mainstream media, we work hard in our free-time outside of our regular jobs to tell the other side of the story and produce content like this. If you can spare a few dollars, any amount can be selected by donating below or visit the Donate To Diverge page on our site. Thank you in advance.
