
To the public – A safe and effective vaccine is one where people don’t get hurt, the vaccine prevents people from getting deathly ill and prevents the number of cases from surging. To ensure this happens, the clinical studies must be organized in a way to ensure that these outcomes are met – but they aren’t, at least not according to an associate editor of the British Medical Journal Peter Doshi.
Peter Hotez, dean of the National School of Tropical Medicine at Baylor College of Medicine in Houston had to say regarding the clinical trials;
“Ideally, you want an antiviral vaccine to do two things . . . first, reduce the likelihood you will get severely ill and go to the hospital, and two, prevent infection and therefore interrupt disease transmission.” This seems pretty straight-forward so far, doesn’t it? Peter Doshi then had this to say in his Feature for the British Medical Journal;
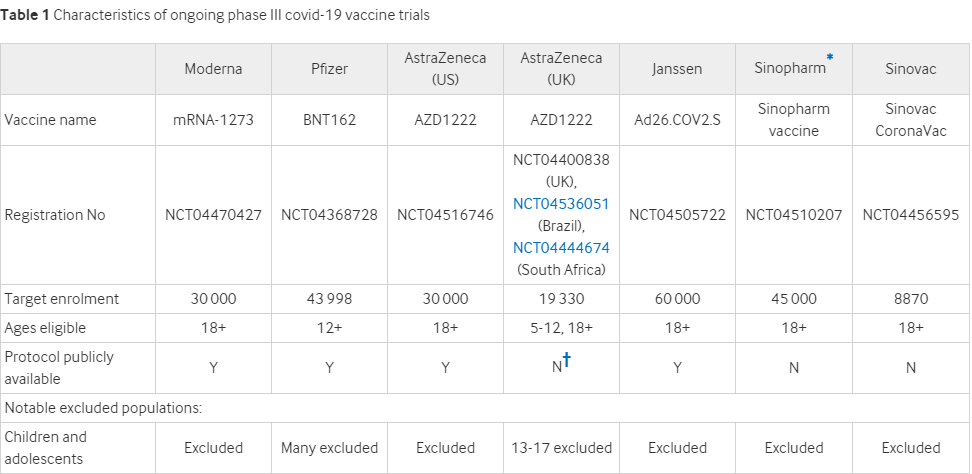
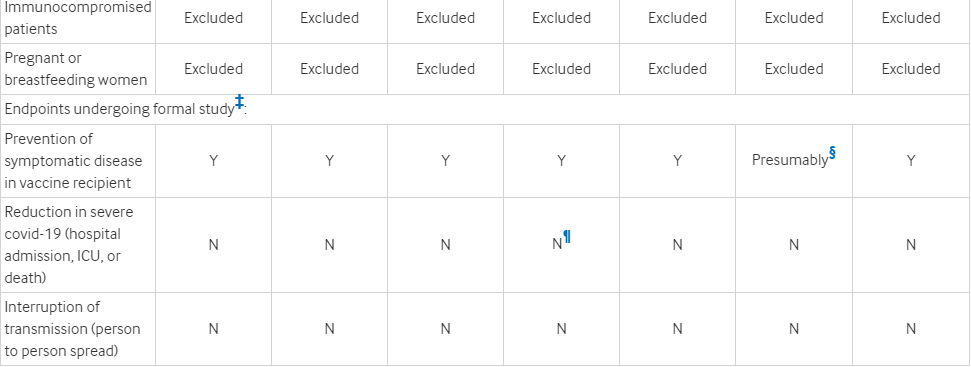
“The current phase III trials are not actually set up to prove either (Table 1). None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.”
“None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths.“
Peter Doshi in his feature for the British Medical Journal
Here is the table listed in the Feature of the British Medical Journal by Peter Doshi.
In a September interview, MedScape editor in chief Eric Topol asked what would be a recorded “event” in the vaccine trials. “We’re not talking about just a PCR [polymerase chain reaction test]-positive mild infection. It has to be moderate to severe illness to qualify as an event, correct?” he asked.
“That’s right,” said Paul Offit, a vaccinologist who is on the FDA advisory committee that may ultimately recommend the vaccines for licence or emergency use authorization.
Here is the issue – that’s not right. According to the feature in the BMJ “all the ongoing phase III trials for which details have been released, laboratory confirmed infections even with only mild symptoms qualify as meeting the primary endpoint definition. In Pfizer and Moderna’s trials, for example, people with only a cough and positive laboratory test would bring those trials one event closer to their completion.”
That’s not exactly comforting considering the vaccine is being rushed and vaccine developers can’t be sued for any harm (including death) they cause to those who take their vaccines. Instead, a separate court was created to protect the vaccine developers from ongoing liability.
The trial’s final efficacy analyses are planned rather after just 150-160 “events” – that is a positive indication of symptomatic Covid regardless of the severity of the illness. Tal Zaks, chief medical officer at Moderna, told The BMJ “The trial is precluded from judging [hospital admissions], based on what is a reasonable size and duration to serve the public good here.” He then said it would take to long to run their trials in a way that measures this;
“Would I like to know that this prevents mortality? Sure, because I believe it does. I just don’t think it’s feasible within the timeframe [of the trial]—too many would die waiting for the results before we ever knew that.” It’s an interesting point that seems to have been debunked with the all-cause mortality statistic by Denis Randcourt of the Ontario Civil Liberties Association.
In Randcourt’s Research Gate publication he said “The latest data of all-cause mortality by week does not show a winter-burden mortality that is statistically larger than for past winters. There was no plague.” – Denis Randcourt
What about stopping transmission of the virus?
Chief Medical Officer at Moderna Tal Zaks had this to say “Our trial will not demonstrate prevention of transmission,” Zaks said, “because in order to do that you have to swab people twice a week for very long periods, and that becomes operationally untenable.” So let me get this straight – you can’t check to prove it will stop transmission because its operationally untenable? What the hell are you developing the vaccine for then?
The Moderna Chief Medical Officer continued to reiterate the “operation realities” of the vaccine trial. ““Every trial design, especially phase III, is always a balancing act between different needs,” he said. “If you wanted to have an answer on an endpoint that happens at a frequency of one 10th or one fifth the frequency of the primary endpoint, you would need a trial that is either 5 or 10 times larger or you’d need a trial that is 5 or 10 times longer to collect those events. Neither of these, I think, are acceptable in the current public need for knowing expeditiously that a vaccine works.”” I bet many would beg to differ.
Zaks then goes on to say that in order to do a trial that would show these outcomes approximately 300,000 participants would be needed and funding in the range of 500 million to a billion. Where has all the money gone that our governments have spent on these vaccines? Instead of doing a proper study, our government has spread the funds thin in hopes they would find a “vaccine” that doesn’t prove even prove its effectiveness in preventing Covid!
No surprise from our Prime Minister
Our Prime Minister has been dishing out billions of dollars for research on a vaccine, and has reserved enough doses for the Covid vaccine to inject every Canadian citizen 7 times over once available. It apparently has never occurred to our Prime Minister to make sure it actually does what the public expects it to – that is to protect the citizens of Canada from severe outcomes and to reduce infections. It only makes sense to have this many vaccines on hand when you consider yourself a global citizen like Trudeau, who plans on giving away Canada’s extra vaccines to “poor nations.”

“OTTAWA/GENEVA – Canada, which has reserved enough doses to vaccinate residents against COVID-19 several times over, is in talks with other governments about a plan to donate shots to lower-income countries, according to three sources familiar with the matter.” – New York Post
More concerns outlined
Harvard drug policy researchers Jerry Avorn and Aaron Kesselheim recently wrote in JAMA “Finding severe rare adverse events will require the study of tens of thousands of patients, but this requirement will not be met by early adoption of a product that has not completed its full trial evaluation.” Feel comforted about the vaccine yet?
The BMJ’s feature continues on the trial concerns stating “Covid-19 vaccine trials are currently designed to tabulate final efficacy results once 150 to 160 trial participants develop symptomatic covid-19—and most trials have specified at least one interim analysis allowing for the trials to end with even fewer data accrued.”
Imagine injecting potentially hundreds of millions of people on the results of 150 people – no need to imagine that’s the plan for the Covid vaccine.
“Imagine injecting potentially hundreds of millions of people on the results of 150 people – no need to imagine that’s the plan for the Covid vaccine.”
Greg Staley – Diverge Media
What is deemed a success in the vaccine trial study?
Where does the 90% effective number for the vaccine come from? Well it appears to come from the following “Moderna, like Pfizer and Janssen, has designed its study to detect a relative risk reduction of at least 30% in participants developing laboratory confirmed covid-19, consistent with FDA and international guidance.”
What is relevant risk reduction?
“In epidemiology, the relative risk reduction (RRR) or efficacy is the relative decrease in the risk of an adverse event in the exposed group compared to an unexposed group.” In this case, that would mean simply a reduction in symptomatic symptoms of Covid – not hospitalizations, not ICU numbers, but symptoms. Only a 30 percent relative risk reduction would be required to be a success in the eyes of the study. This is where your 90% effective number comes from!
Only a 30 percent relative risk reduction would be required to be a success in the eyes of the study. This is where your 90% effective number comes from!
Greg Staley – Diveerge Media
In the BMJ feature Doshi writes “Number two, Zaks pointed to influenza vaccines, saying they protect against severe disease better than mild disease. To Moderna, it’s the same for covid-19: if its vaccine is shown to reduce symptomatic covid-19, it will be confident it also protects against serious outcomes.” You know what they say about assumptions.
This doesn’t address what happens when someone who has taken the vaccine gets symptomatic Covid-19. It doesn’t address if it reduces the risk of hospitalizations or adverse effects. It merely assumes that one (reduction in symptomatic Covid cases) leads to the other. This can’t be the benchmark for success.
This point is further discussed below.
Influenza vaccines show flaws in the Covid study design
“Although randomised trials have shown an effect in reducing the risk of symptomatic influenza, such trials have never been conducted in elderly people living in the community to see whether they save lives.
Only two placebo controlled trials in this population have ever been conducted, and neither was designed to detect any difference in hospital admissions or deaths. Moreover, dramatic increases in use of influenza vaccines has not been associated with a decline in mortality.”
Re-cap
- The study designs for Covid vaccines don’t measure for reduction in cases or severe illness that lead to hospitalizations and ICU visits
- The measure of success for these studies is if they reduce symptoms in symptomatic people by at least 30%, hence the 90% effective numbers Moderna and Pfizer have released
- The studies don’t follow the vaccines ability to prevent infection to others (likely why they try to justify the “no new normal after vaccine”)
- For proper studies to be done at least 300,000 participants would be needed
- no influenza vaccine randomized controlled trials show a decline in mortality with increase of infleunza vaccines (only 2 studies exists)
- They assume if they can reduce symptoms it will reduce severe cases from the virus (don’t assume – you need to know)
I have never been so angry while writing an article. I fought back tears as I asked myself the question “what are we developing this vaccine for if it isn’t to prevent death and infections?” This screams of corruption – all made possible on the basis of the fear that government has constantly pushed in regards to the Covid-19 virus.
Who will speak out on this? Who will champion this information? We need help – we need you to share this as far and wide as you can. Send it to every politician willing to listen. Send it to your healthcare practioner. This is information the world needs to know! Regardless of your feelings on the vaccine itself – this isn’t a recipe for a good vaccine.
Diverge Media is an independent media outlet dedicated to bringing you the stories that matter. We don’t, and will not ever accept funding from government. We rely on our readers and viewers to support our work. If you would like to support us – please do so by donating in the form below! Merchandise will be available just before Christmas! Throw us a message to inquire!
